Sometimes, life doesn’t go how you’ve planned. We get it. A pain in your knee limits your summer hiking plans. A torn rotator cuff leads to a surgery and time off you haven’t planned for. Sometimes your aches and pains don’t necessarily limit your participation in an activity, but they don’t allow you to do things the way you would like to do them. Pain and discomfort come in all shapes and sizes. And not only that, but it happens to the best of us!
Take my case, for example. I was clicking along, training for a trail-running half marathon that is happening this October – the Durango Double that begins and finishes right behind our clinic that we love to sponsor and volunteer for! But, there were a few bumps and snafus that happened with my busy life schedule that happened to derail my training, which led me down a bumpy road to injuring myself due to poor training habits coupled with a pre-existing condition that I was not addressing the way I should have been. You may think, “But, you’re a PT – you should know better!!!” So, in the end, I’m taking a time-out from running to focus on my body in the way it needs to be focused on. What better way to do that then by surrounding myself with smart, caring and trustworthy PTs (AKA my colleagues here at Tomsic PT!) that can help guide me along my path to rehabilitation so that I can keep up in participation of trail-running endeavors for many years to come!
Sneaking in some exercises between patients
The neat thing about that concept is that there is research that has shown the powerful effect on the relationship between patients and physical therapists on treatment outcome in patients with low back pain.1 Sure, a well-trained PT is worth their weight in gold when they can recognize what is happening in your body that is contributing to your pain and, even more importantly, what needs to be done to help reduce your pain and discomfort in order to meet your goals. But, beyond having the ability to identify and treat your problems appropriately, the relationship- or therapeutic alliance- that is built between you and your PT may predict how much better you will get.1 Specifically, the therapeutic alliance depends on three things: (1) the therapist-patient agreement on goals, (2) the therapist-patient agreement on interventions (AKA treatment choices), and (3) the affective bond between patient and therapist, which refers to the trust and confidence that the treatments will bring the patient closer to their goals.1
Research has demonstrated that higher levels of therapeutic alliance were associated with greater improvements in perceived effect of treatment, function, and reductions in pain and disability.1 I just find it fascinating that the relationship we love building with our patients is not only fun in our small community, but it actually helps our patients get even better than they would have if we didn’t have a strong alliance built during our time together! Getting on the same page with your goals, the treatments we are offering, and how confident we are in how those treatments can improve your conditions is integral to having a successful rehabilitation of your problem. Even though this research focused specifically on low back pain, my hunch is that we can extrapolate this information to other areas of pain and discomfort as well. I feel fortunate that I am surrounded by empathetic and knowledgeable PTs to help guide me through my own issues, and I hope that each and every one of our patients realizes the importance in creating these relationships with each other!
Ferreira PH, Ferreira ML, et al. The Therapeutic Alliance Between Clinicians and Patients Predicts Outcome in Chronic Low Back Pain. Phys Ther. 2013; 93:470-478.
I always love finding out new information regarding the impact of running on our bodies. As a runner, I know the love-hate relationship that I have with running as sometimes it feels like the thing that can cure my ailments and other times it feels like it may cause them. From some of my older patients, I have heard everything from, “Running is the best activity for my heart that has kept me strong throughout my life,” to, “I wish that I never started running because it ruined my knees.” With so many varied experiences, the question often comes up about whether or not running is beneficial or detrimental long-term. As it turns out, not only me and my patients are asking this question, but researchers are as well.
Enjoying the beautiful flowers and mountain views on a July trail run- not a bad backdrop for a run!
A recent systematic review and meta-analysis, which are quality ways to assess all of the available data regarding a specific question, sought to find out if there was any association between running and hip and knee osteoarthritis, which is a condition where your joints undergo degenerative changes that may cause pain and dysfunction.1 And even beyond that, the researchers wanted to find out if the running intensity and history of years running had any influence on this association.1 The researchers ended up being able to analyze 25 studies, which gave them a good sample of information to help them answer their questions.1
Getting out for a run in the high country surrounding Durango!
Overall, this analysis of studies found that running was not necessarily associated with osteoarthritis and, in fact, recreational runners had lower odds of hip and/or knee arthritis when compared to competitive runners and sedentary non-runners.1 In terms of years running, the people that ran less than 15 years had a lower association with osteoarthritis than those who ran more than 15 years.1 That being said, most of the studies that looked at running for more than 15 years were focused on competitive runners, who already had higher odds of developing arthritis, and they were unable to find conclusive information on recreational runners that ran for more than 15 years.1 The definition of competitive runners were runners that were reported as professional, elite, or ex-elite athletes, but the amount of miles of running was not necessarily described.1
So, what’s the take-away? It seems that recreational runners may be better off for having lower odds of developing hip or knee osteoarthritis than those who run competitively and those who don’t run at all and are more sedentary in general, especially if they run for less than 15 years total.1 As far as knowing about the impact of running recreationally for more than 15 years, there is not quite enough information to tell!1 There are more factors that go into running that can potentially affect your joints and pain, which are factors that PTs are specifically trained to identify and treat. If you have questions about how running might be impacting your joints, make sure to see a PT to have your running form and strengths/weaknesses analyzed to find an individualized approach to your issues.
Alentorn-Geli E, Samuelsson K, et al. The Association of Recreational and Competitive Running with Hip and Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Journal Ortho Sports Phys Ther. 2017;47(6):373-390.
\It’s May in Durango, which means cycling season is officially in full throttle! With these month’s races such as 12 hours of Mesa Verde and the Iron Horse Bicycle Classic road and mountain bike races, there are a lot of locals hitting the pavement and the dirt to start getting their miles in. As PTs, we see a lot of folks whose main goal is to be able to bike without any issues. There are always discussions on bike posture and what is the “right” position for each body, for which there is not a carte blancheanswer. That being said, there are some general guidelines that may be undertaken for cycling that may help you have a more successful season.
John showing off his bike position at 12 Hours of Mesa Verde
As it turns out, a slim majority (51.5%) of cycling-related injuries are related to overuse, and low back pain is the most common of these types of injuries.1 These injuries can cause lost time on the saddle and require medical intervention, so they are important to pay attention to and, more importantly, to figure out how to prevent. For road cyclists especially, a flexed (or bent over) spine position is used in an attempt to create proper aerodynamics which might translate toward increased speed and efficiency, which are both desired goals for racers and non-racers alike.1 A recent systematic review, which is an analysis of multiple studies, sought to determine if there is any relationship between body positioning and spine muscle activity in cyclists with low back pain that wasn’t brought on by trauma.1 The researchers also wanted to find out if bike fit affects these factors, so that cyclists can have more guidance on how they should be set up on their bike in order to feel their best.1
After reviewing eight studies, the researchers found that there is evidence that supports the idea that muscle activation imbalances in your core muscle group are risk factors for low back pain in cyclists.1 The studies also support the idea that there is some relation that sitting in a prolonged, flexed position during cycling is related to low back pain.1 Changes such as a well-balanced core muscle activation program as well as changing your positioning on your bike to one that is less bent-over may very well decrease your risk of developing low back pain.1 Specifically, a lower handlebar position that requires your back to flex more may set you up for further issues.1 Physical therapists are specially equipped to assess and help you refine your ability to activate the muscles in your body and especially in the core muscle group. We also love to assess bike positioning in order to find the best position for your body and recommend changes that will either prevent or reduce low back pain. If you are a cyclist and you are currently experiencing back pain or would like to know if you are at risk for developing back pain and what to do about it, call us to schedule an appointment with one of our specialized PTs.
Streisfeld GM, Bartoszek C, et al. Relationship Between Body Positioning, Muscle Activity, and Spinal Kinematics in Cyclists With and Without Low Back Pain: A Systematic Review. Sports Health. 2016;9(1):75-79.
You may notice that we usually have one or two students around the clinic at any time. As a physical therapy clinic, we get the opportunity to host Doctorate of Physical Therapy (DPT) program students from all over the nation as well as undergraduate interns mostly coming to us from Fort Lewis College.
The staff with our 2016 Regis University DPT student, Vickie
The DPT students come here seeking an enriching, hands-on experience in order to put the skills they have gained during their didactic curriculum into practice in a real-life setting. Their time with us, whether it be a short 6-week rotation up to a longer 12-week rotation, is supposed to be the time where a lot of the actual learning happens, especially in learning how to treat patients with their hands and communicate effectively, all with the end goal of making you, the patient, feel and function better!
Jeff with our 2016 Idaho State University DPT student, Kevin, working to help a runner after a race
The undergraduate interns, which are mostly exercise physiology majors from Fort Lewis College, are utilizing their time here to learn more about the profession of physical therapy. This helps guide many students to decide if they want to pursue further graduate education in order to become a physical therapist, versus other healthcare professions that they may be interested in. These students are not so much hands-on like the DPT students, but they are in more of an “observation and shadowing” mode so that they can assess the day-to-day of a physical therapist.
Laura posing with her alma mater’s 2016 University of Utah DPT student along with Scott Ward, the dean of the Physical Therapy program
Regardless of which type of student we are hosting, the benefits to the clinicians are immense. Not only does hosting a DPT student end up in higher productivity levels for the provider1, the clinical instructor that is assigned to the student gets to refine their clinical reasoning skills by being challenged to teach and explain why they are doing what they are doing. As new research and evidence regarding best physical therapy assessment and treatment comes out and is taught in professional-level DPT programs across the nations, we get to keep our pulse on the latest and greatest research that may change the way we practice for the better in order to ultimately get each patient better, faster. Also, the patient gets to become much more of a learner as to the “why” of PT, as they get to take part in the learning experience that is very much reciprocal between each clinical instructor and their student. All in all, it is a “win-win-win” situation for the three people involved!
Carmen, our 2017 Regis University DPT student, refining her manual therapy skills
Next time you are in the clinic and you get to meet one of our students, make sure to take time to appreciate the learning and benefits involved in their presence in our clinic!
Pivko SE, Abbruzzese LD, et al. Effect of Physical Therapy Students’ Clinical Experiences on Clinician Productivity. Journal of Allied Health. 2016;45(1):33-40.
It may feel like has Spring has already sprung here in town, but up in the high-country there are still plenty of days left to participate in one of our area’s favorite wintertime activities: snowshoeing. For those who may not necessarily like to ski or snowboard, snowshoeing is a great way to get into the great outdoors in the winter as well as a great way to get your heart rate up. Whether it’s a gently paced walk on a traversing trail, a more steep incline and decline (with a couple bouts of sliding on the way down!), or a running race on snowshoes (yes, those do exist!), folks of all levels can participate in this activity. In fact, a survey in 2006 found that approximately 5 million people participate in snowshoeing, and they estimate that this number is growing.1
Snowshoeing for any age!
A fairly recent study from researchers at CSU in Ft. Collins and a university in Australia wanted to get down to the nitty gritty of “how we move” in snowshoes AKA the biomechanics of it.1 I won’t engage you in all of the intricate details, but in general we tend to stand in a more flexed, or bent, position of our hips and knees, pull our hips into more of a bend while swinging our legs forward, and start to point our toes a little sooner as we are about to put our foot on the ground while stepping forward.1 These changes in the way we move while snowshoeing, namely the semi-“crouch” position we end up in, are likely the main reason that we expend more energy versus overground walking as it requires more use of our leg muscles and is less efficient than the normal heel-to-toe walking that we usually do.1 For something that expends your energy twice as much as walking a level ground, snowshoeing turns out to be a great way to exercise during those winter months when you’re feeling a little more cooped up!1 So, hopefully you are able to get out there and enjoy a little bit more of the high-country snowshoe trails before the snow melts this spring and don’t hesitate to talk to your physical therapist about the value of snowshoeing.
Browning RC, Kurtz RN, Kerherve H. Biomechanics of walking with snowshoes. Sports Biomechanics. 2012;11(1):73-84.
One of my first days in the backcountry this year. It sure was fun, but I was sore!
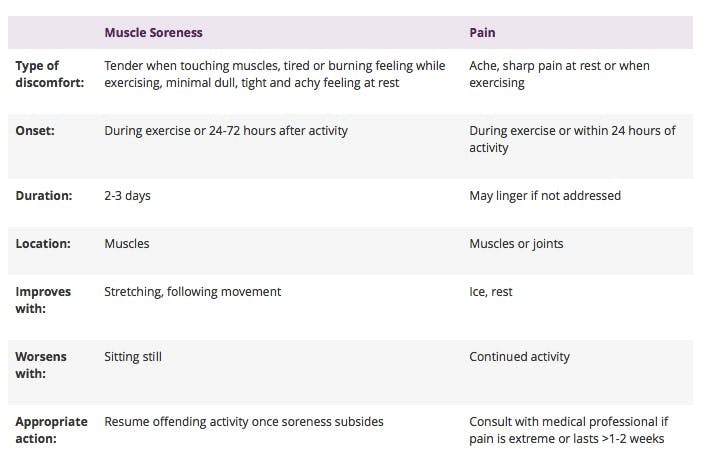
The American Physical Therapy Association’s (APTA) website for the public, called Move Forward, just came out with a great article about the difference between soreness and pain.1 As PTs, we get questions all the time about how much soreness is “normal” during various exercises. Although you are expected to feel some discomfort either during or after exercises, the old phrase “no pain, no gain” isn’t always true, either. While it is true that you do need to push your body to achieve gains, the push has to be at an appropriate level, which is different for each person depending on their age, current activity level, and strength, among other factors.1 As you continue to push your body in an appropriate fashion, your threshold for activity should increase and increase.1
Think about it like your first day back on skis for the season: for most of us, the first day back is usually a “mellow” one, where you hit up a series of relatively easier runs with interspersed breaks to “warm-up” your legs and get used to the motions required to make it safely and gracefully down the slope. After this first day back, you may experience some delayed muscle soreness for 1-2 days after skiing. Then, on your second and subsequent days back, you may take less breaks between runs and choose more and more challenging runs, with just the same amount of soreness as after the first day (or no soreness) as your body gets used to the challenge that you are providing. However, if you take your first day back on the slopes as a non-stop, quad-crushing day with mogul runs over and over again (and, most importantly, you weren’t prepared for it), you might pay for it later with a higher level of soreness that doesn’t quite go away after a couple days. That would be called pain. The Move Forward website broke it down in an easy-to-read table here:
For more information on telling the difference between pain and soreness, consult with a physical therapist today to make sure you are playing hard within your body’s limits!
Soreness vs Pain: What’s the Difference? Move Forward. American Physical Therapy Association. https://www.moveforwardpt.com/resources/detail/soreness-vs-pain-whats-difference. Accessed on December 5, 2016.
Our goal as physical therapists is to help people feel better, move better, and ultimately live better. One way that we achieve this is through manual therapy (AKA hands-on) treatments, including manipulations (faster, low-amplitude movements) and mobilizations (slower, low- to high-amplitude movements). If you have ever participated in physical therapy, chances are that your PT did some form of manual therapy to work on, or near, the parts of your body where your pain was. You likely walked out of that treatment feeling less pain, as that would have been the goal of the PT’s treatment. Did you ever wonder to yourself, “How did that work to help me feel better???”. You’re not alone.
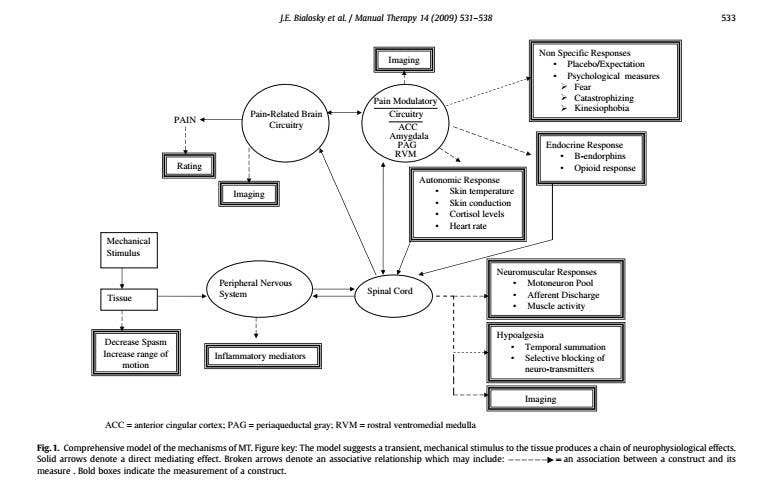
This is a question that the PT profession as a whole has been working toward answering over many years through the undertaking of extensive research. Although there is no “one” answer for how manual therapy specifically works to reduce pain and improve overall function, the studies have shown that, rather, there are many moving parts that contribute to the effectiveness of manual therapy treatments. A model for this was created by Dr. Joel Bialosky, et. al, back in 2009 with the intent of guiding future studies and serving as a basis of the knowledge we have about how manual therapy works so far.1
I’d like to take this opportunity to break down the model above so that it makes more sense to anyone reading this, regardless of your background in health sciences.1
When manual therapy (the “stimulus”) is applied to a certain part of your body (the “tissue”), the immediate effect is decreased spasm of the muscles in the area and increased motion.
This stimulus being applied sets off a cascade of effects, starting with the “peripheral nervous system” (all of the nerves in your body besides those in your spinal cord and in your brain). An effect of this stimulation is that cells that help attack inflammation are sent to that area (“inflammatory mediators”).
Then, the information is sent to the main nerve conduction track between your body and your brain (the “spinal cord”). From here, a whole host of proposed effects occurs, including improved muscle activity of the area that was worked on and decreased pain (“hypoalgesia”).
After the information gets to the spinal cord, a feedback loop with the brain begins, which includes changes related to pain, involuntary nervous system (“autonomic”) responses such as changes in stress hormone levels, heart rate, and skin temperature, endorphin and opioid responses (the “feel-good” hormones), and psychological responses to the treatment including expectation and the placebo effect.
All of that boils down to the fact that, after a PT has performed a specific-to-you manual therapy treatment, you typically feel better! This model just demonstrates that there are a lot of factors that play into the why of you feeling better, and research in this subject continues to evolve so that we, as PTs, can better understand how our treatments help you feel better. If you have more questions about how manual therapy works to reduce your pain, make sure to come in and speak to a physical therapist to learn more and benefit from this treatment.
Bialosky JE, Bishop MD, et al. The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Man Ther. 2009;14:531-538.
Is anyone else as ready as I am to see those first flurries of fall come down? When the weather starts changing and ski swaps start becoming a regular weekly occurrence, I’m sure I’m not the only one that starts dreaming of powder days at the resort and in the backcountry. In fact, in the US alone, over 18 million people skied or snowboarded at least once during the 2011-2012 winter season, and with the rate of growth in those sports we can only assume that number has grown over the past couple of years.(1)
We all know the risks of skiing and snowboarding that are present, as it’s rare to come across someone who doesn’t have an “epic” yard-sale story. I’ll never forget the day last winter that I hit a patch of “brown snow” in the backcountry and completely went flying head over heels as my momentum had been completely halted due to the snow friction transition. Luckily, I just stood up, found my skis, and shook off the snow that had accumulated in my jacket to continue the rest of my journey down to the car and a warm drink. Unfortunately, not everyone is so lucky, and as PTs in a mountain town we tend to see our fair share of skiing and snowboarding injury aftermaths.
A recent study from The Orthopaedic Journal of Sports Medicine compared surveys that were taken at Big Sky Resort in Montana in 1996 and 2013 to see how the amounts and types of skiing and snowboarding injuries have evolved over time as the sports have become more and more popular.1 In 1996, 85% of the injured participants surveyed were skiers and this number dropped to 73% in 2013, showing that there were more injured snowboarders (possibly related to more snowboarders being on the hill).1 The average age of those being injured stayed 34 years old between the two time periods but, in general in the survey, injuries were occurring more often for those in the 46-55 year age group.1 Some great news is that the number of participants wearing a helmet jumped from only 6% in 1996 to 84% in 2013!1 It seems like people are wising up with helmet use in an effort to reduce their risk of head injury.
In terms of what body parts are more frequently injured in skiers, it looks like the knee still is the winning joint totaling to about 28% of all injuries both in the past and more recently.1 However, the proportion of shoulder and arm injuries increased significantly for both skiers and snowboarders, and those types of injuries continue to be the most common in snowboarders totaling 33% of all injuries in 2013.1 Also of note, the number of injured participants who had never received any professional instruction increased from 19% in 1996 to 30% in 2013, and the number of injuries that occurred while using rental equipment increased from 27% to 39% in the most recent survey.1 This suggests that more infrequent and novice skiers are the ones that are the most likely to be injured.
Granted, this is only based of surveys taken from one ski resort in the country. However, it is interesting to see the trends that have occurred over the years as these sports continue to evolve and grow in participation. Hopefully you will be one of the lucky ones that will avoid injury this coming snow season. However, if you do happen to be one of those folks that sustains an injury while out on the hill this year, know that you can count on a qualified group of physical therapists to get you back out as soon as possible to enjoy another powder day.
Patrick E, Cooper JG, Daniels J. Changes in Skiing and Snowboarding Injury Epidemiology and Attitudes to Safety in Big Sky, Montana, USA: A Comparison of 2 Cross-sectional Studies in 1996 and 2013. Ortho Journal Sports Med. 2015;3(6). doi:10.1177/2325967115588280
This is the final installment of the squat series, where we will discuss the myriad of ways you can incorporate squatting into your workout. In part one we discussed the many health benefits that simply squatting provides throughout the day. In part two we discussed some of the fine nuances of form that make a proper squat and those that are detrimental in terms of poor form. As we discuss the various ways that you can incorporate squatting into your workouts, remember that you are in charge of your body and how it works. Many of the squats that we will discuss will be fine for a person to perform if they own perfect movement mechanics but for someone who is movement challenged these squats may very well aggravate your system.
I will breakdown the squatting by starting with the least challenging or the least functional squatting and then slowly progress to the most challenging and the most functional. Notice that I lumped the words challenging and functional together which was done on purpose. Typically, but not always, a movement that is very challenging to perform also has a high correlation to function. Full body movements that are challenging to the central nervous system are such that the exercise becomes self limiting. Mindless repetitions cannot be performed and these self limiting exercises seem to help asymmetries, movement pattern problems and minimize the chance of incurring a repetitive trauma type injury. Are you ready??? Here we go.
Barbell Back Squat
The barbell back squat has been around since man invented the barbell. This type of squat is the least functional for a number of reasons. The first being – what type of daily activities do you perform where you have a load on your back and you repetitively squat up and down. Rarely if ever. The second issue is that with the back squat you can have absolutely horrible form and still complete the squat which of course is a bad idea to continue this habit. Second, because the bar is on your back you can perform this type of squat with fairly heavy loads and again still complete the movement which will place unnecessary stress on your spine. Third, because you can lean forward with the weight on your back, you increase the lever arm on your spine which ramps up the stress on the lower lumbar discs and, again, place unnecessary loads on the spine. Many traditional athletes and coaches still swear by this type of squat as being the holy grail of training but in recent years we have seen many new age coaches understand the limited carryover of this type of squat to actually improving their athletes performance on the field. I should mention that the picture that I choose above displays horrible form yet the squatter was probably successful in lifting the weight. Personally, I would never encourage anyone to perform this type of squat.
Barbell Front Squat
The barbell front squat is a common exercise to those who know the Olympic lifts. It is a much more challenging exercise than the barbell back squat and for many reasons a much more functional exercise. First by the nature of having the barbell across the front of the shoulders and resting on the fingers much less weight can be used than during the barbell back squat. Since less weight can be used during this squat, there is less strain on the lower back and that is always a plus. Second, because the weight of the barbell is resting on the shoulders and fingers the spine or trunk must be upright and if the trunk starts to lean forward you are surely going to drop the weight forward. The fact that the spine/trunk must stay very upright also places less strain on the lower back. Third, because the shoulders, elbows, wrists and fingers are stretched to maintain the front rack position this helps maintain a level of flexibility in these joints that is not stressed in the barbell back squat. This exercise has more carryover to daily activities then the barbell back squat. I recommend this type of squat even for beginners.
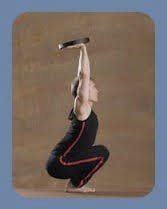
Barbell Overhead Squat
The king of barbell squat exercises. This exercise is the most challenging barbell squat exercise because the arms are now holding the entire weight of the barbell in an overhead press position. This type of squat demands maximum thoracic extension, scapula mobility and shoulder stability. Plus while the thoracic spine is staying in extension the lumbar spine is slightly flexing at the bottom of the squat requiring a high level of core flexibility and stability. This type of squat demands thought while you are performing the exercise so it is very central nervous system (CNS) intensive. You can not perform mindless reps of this exercise while watching the TV at the gym, the overhead barbell squat requires total focus. When you become proficient in performing this exercise with heavy weight, normal daily activities will seem like a breeze. This exercise will also carry over into improving other functional activities such as sprinting and jumping. I recommend this type of squat for intermediate level lifters.
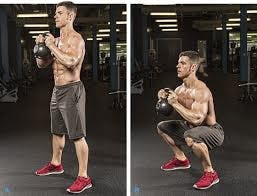
Goblet Squat
The Goblet Squat is probably the most functional dumbbell or kettle bell based squat. Look at the position of the kettle bell, it is exactly in the same position you would be carrying an item that you needed to squat down to the floor with. While the overhead barbell squat requires more coordination, flexibility and stability, the goblet squat more closely resembles a daily activity therefore has more carryover to enhancing a movement you are more apt to perform. That is what training is all about. Proper form in the goblet squat allows an upright trunk which stays in neutral allowing the hips, knees and ankles to perform all the motion. This is congruent with the principles we discussed in the Squat Part 2. If you have never squatted before as an exercise this is probably the best introductory weighted squat for you to incorporate in your training. I highly recommend this type of squat even for those who have never lifted a weight before in their life.
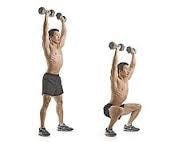
Dumbbell Overhead Squat
The Dumbbell Overhead Squat is another variation of the overhead squat. Obviously holding separate weights in each hand instead of a bar places more challenge and demand on this exercise and that is a good thing. If you have an asymmetry in one shoulder vs the other this type of squat with typically expose that issue. That is why these challenging and purposeful exercises are wise to perform periodically because they help you realize a movement issue by challenging the CNS and your musculoskeletal system. A barbell back squat will not challenge the system like this squat will and therefore a shoulder or trunk or hip problem might go unnoticed. I perform this type of squat once a month as a warm-up for heavier barbell overhead squatting simply to test my movement. I recommend this type of squat as a warm-up or test but not as a heavy exercise unless you are an experienced lifter.
Pistol Squat
Life is not all about being on two feet all the time. Think about sports, are you on both feet all the time. Rarely! The majority of sports require running, sprinting, cutting, decelerating, hopping or jumping. This predominantly requires each leg to be able to perform independently of what the other leg is doing. This requires near perfect trunk control to be able to balance and coordinate the action of standing on one leg and allow full weight bearing through maximal range of motion. This is not a beginner exercise! Only those desiring maximal athletic performance and bulletproof joints should perform this exercise. As a prerequisite you should be able to perform all of the above squats with at least bodyweight as resistance prior to trying the pistol squat. If you have any known back, hip, knee, ankle or foot malady this squat is not for you. This squat should also be performed without resistance first to see if you own the balance, flexibility and control required. Then once you display competency external resistance can be added. The risk and reward for this squat should only be accepted for the extreme athlete therefore I am highly cautious in recommending this exercise unless I have observed your movement level.
The Candle Squat
Are you serious? The candle squat as created and probably only able to be performed by Jerzy Gregorek. For those of you unaware of this man’s ability, I implore you to visit The Happy Body website where Jerzy outlines a baseline level of nutrition, flexibility, strength and stability that is unparalleled. If you were looking for the gold standard in squatting than this is platinum. This gentleman’s ability to move makes me absolutely jealous. A picture is worth a thousand words so I will stop writing. If you are even remotely close to possessing the ability to perform this squat then stop reading my blog as reading any further could only surely cause you some level of dysfunction and we wouldn’t want that.
Conclusion
To summate all that we have discussed in this three part series on the squat, I must confess that there is surely an awful lot that I have not discussed or by constraint omitted. The subject of squatting is vast and the breadth of information fills whole books. The important point that I wanted to convey over the past few months on this blog is the importance of correct daily squatting.
Just like your motor vehicle requires oil changes, tire air pressure checks and other routine maintenance your body requires daily squatting as maintenance for baseline musculoskeletal health. Your body requires other daily movement different than squatting to maintain its health as well. Dr. Kelly Starrett has come to the conclusion that 10 minutes a day in the deep squat is a good baseline. Proper daily squatting is similar to eating whole food for your nutrition and getting eight hours of sleep a night in terms of health for your body.
I encourage readers to educate themselves on their own performance by having your movement assessed by a professional. Having your movement assessed by a trained individual can be enlightening, eye opening and explain if you have been consistently injured or stuck in a rut with your performance. Please call our office and I will be glad to run you through a functional screen. Two people who possess near perfect movement ability and should therefore be emulated are Jerzy Gregorek, who was mentioned earlier, and Steve Cotter of IKFF and kettle bell fame. Both of these people can be found on YouTube and their websites on the internet. Here’s to your health, happy holidays and happy new year!
In this second of three part series on the squat we will discuss foot placement, form and posture which aid in making a more efficient squat. In the first part of this series I discussed some of the important reasons as to why we should squat. Before I delve into specifics about aspects of squatting I want to remind the reader of some important details. First we all learned how to place ourselves in the squat position by starting on the ground first and allowed trial and error to “find” our own perfect squat form. No teacher stood next to us giving us cues or suggestions or tips—we simply kept trying and trying until we “got it” and we probably smiled when we achieved our first squat. My point is that it will truly take “you” to take yourself through trial and error and possibly endless repetition to slowly improve your squat. No one can do this for you but you.
Chances are you are past your teenage age years if you are reading this and years of sitting in classrooms, traveling in cars, making poor exercise choices and the litany of other daily environmental dysfunction has tarnished your once stellar squat. You are not alone. Very few young people today even in their college years possess an unblemished squat. Whole movement like a squat demand that multiple joints, muscles, fascia, motor control and lack of pain are working in total harmony. That ankle sprain you experienced in middle school, the torn ACL you injured on the ski slopes or that hip pain you developed while training for a marathon might already predispose you to a poor squat. The take away here is to acknowledge if you already are aware that you possess a movement problem. How well do you know yourself?
I’ve met people who know how fast it will take them to hike up Smelter Mountain within a few minutes but have no idea if they can squat well. Similarly, some people are oblivious to how well they can lunge or how well they can balance on one leg. Can you stand with your knees straight and touch your toes or touch the floor? Knowing how you move with just the force of gravity and the ground underneath you is the most basic movement information you should know about yourself. Why? Because from the second you left your mothers womb till about 12 months of age that is exactly the environment in which your brain learned how to move.
Your body, gravity and the ground- let the learning begin!
Yes you learned how to move. Most of the other primates and all other mammals popped out of mommy and within minutes to hours are up on their feet and walking around. Their nervous system was hardwired with the basic locomotion software to get them moving within day 1. You and I and every other human that ever walked this earth and every human that will ever walk this earth learned how to move through progressive patterns building on each other and culminating into efficient walking. Your brain is learning every second of the day you are awake. You are either learning something new every second or reinforcing something you already knew. You can always teach an old dog new tricks as long as the old dog wants to learn them.
Our brains’ awesome ability to continuously learn is a double-edged sword. It’s double-edged, because you can’t cherry pick what you want it to learn and what you don’t. What ever you are experiencing at the moment your brain is taking in the experience and learning something from it. When we were babies and learning to move we were full of mobility and a desire to move. We didn’t have sprained ankles, torn ACLs or unhappy hips, we were basically free from dysfunction and our brain learned how to move based on this clean slate. Once we developed handed-ness that was the beginning of dysfunction. The more asymmetrical you are in terms of what one side of your body can accomplish vs the other increases your risk of injury while you perform daily activities. Previous injury to a body part increases your risk of injury. Your brain has learned to overcome this issue.
At the top of the hierarchy about what your brain cares about is not how well you squat. It cares about survival! When you were younger and running around the yard and tripped on your knee you got up, assessed the situation and because your knee didn’t hurt “that” bad you kept running around. Except now instead of running around with flawless gait you are limping a little. Your brain doesn’t care, good or bad, you are experiencing a new way to move, right or wrong, optimal or not—you are still learning and you are learning how to run with a limp. The more you run with a limp the more your brain is learning a new pattern of running and if you continue to run in this new fashion your brain will totally re-write its software pattern. Until, you start running “normally” again and then your brain will re-learn the original pattern and your running pattern should return to its near original efficient pattern. Your brain cares about your survival. If you are still alive and you run with a limp, your brain is ok with that. Are You?
The most amazing thing that scientists have discovered in our universe and you own one! This guy can be your best friend or your worst enemy- be good to yourself!
Why bring up how your brain learns? Because your squat pattern has probably been
slowly progressing into an inefficient pattern through the years or maybe you simply don’t squat at all. That is good news! You have realized your current baseline and since your brain has the ability to learn, you can learn a new and more efficient squat pattern. All you need is the desire and the right path. Let’s see if you are ready!
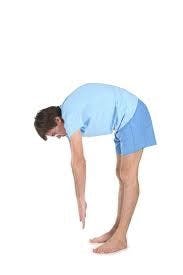
This simple test tells me that you are not ready to squat.
Stand up with your feet together and keep your knees straight. Now bend forward and touch your toes. Can’t reach your toes? YOU are not ready to SQUAT!
Why not?
Your hips are not bending enough. If you try practicing a full depth squat your back will be flexed forward to such a degree that it will be dangerous for your lower lumbar discs. There is a saying in physical therapy that proximal stability allows distal mobility. For every action there is an equal an opposite reaction. Therefore distal mobility allows proximal stability. If your hip joint which is distal to your core is stiff then reflexively your core cannot be stable. I have good news for you. You can still squat but off of a box. Off of a box you say. Does that sound strange. It shouldn’t because you do it everyday and have since you were in kindergarten. What kind of a box am I talking about — a chair!
So if you fall into this category of not being able to touch your toes in standing you need to work on the flexibility of your hips and work on box squatting. Box squatting is like squatting with training wheels on and I have clients squatting off low stools and benches all day long. For those of you that can touch your toes please read on.
Perfect!
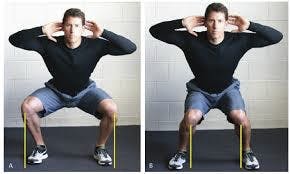
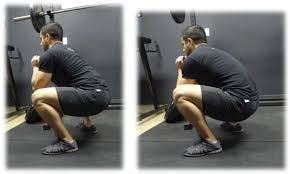
So you can bend forward in standing with your knees straight and touch your toes. Now you are ready to squat down to full depth. Place your bare feet about shoulder width apart or a little wider. Keep your feet facing straight ahead. Start lowering yourself down with a combination of bending your knees and flexing your hips. Try to keep your spine as vertical as you can. As you are lowering down try to actively push your knees outward using your hip muscles. Also as you lower yourself down keep your heels flat on the floor. If this a real struggle or impossible then we need to possibly re-assess matters. There are 3 big aspects of the squat we need to respect. Heels down. Feet facing straight ahead. Knees tracking over toes or tracking wider. Period.
Why do my heels have to be on the ground? When your heel bone, calcaneus, is on the ground then the posterior chain of your body becomes activated. The posterior chain is comprised of all the muscles on the back side of your body. If your heel comes off the ground the base of your support naturally becomes less and you are now performing a balancing act versus a stable squat. If your heel comes off the ground then your knee will pass over your toes considerably and the pressure in your knee can reach dangerous levels. This brings up the conversation of shoes with a raised heel, boots or “heels”. If you are wearing footwear with a raised heel and your job, workout or daily life requires you to squat repetitively expect to experience some anterior knee pain sooner or later. You were designed to walk, stand, squat, lunge, jog, sprint, jump, hike, dance and step all without a raised heel — so stop wearing them!
Heels down, knees happy!
Very fashionable- Let me know how your knees feel when you are 50!
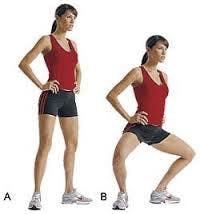
Why do my feet have to face forward? This makes it much easier for your knees to track over your toes or on the outside of your feet. The more your feet toe out the more you have to push your knees out even wider. So if your feet are facing forward when you squat and your knees buckle inward, push your knees out. If you can not because your hips are too weak then stop squatting. If you squat with your knees buckling inward you stand a good chance of injuring your meniscus, medial collateral ligament or your anterior cruciate ligament or a combination of the three. We talked earlier about your brain and the fact that its learning all the time. If you squat with your knees bucking inward and then perform that repetitively then you are learning how to squat poorly and this will create a hard habit to break. Also when you actively use your hips to push your knees out wide and your feet face forward you tend to elevate the arch in your foot— simply another bonus.
There is one caveat.
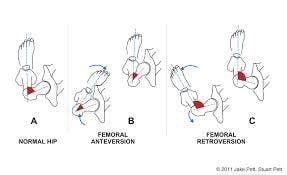
Do you have hip anteversion or retroversion? This is where the femoral neck is rotated forward or backward instead of normal alignment. If this is the case then your knee will naturally be rotated inward in the case of femoral anteversion. If your hip is retroverted then your knee will be facing outward. Similarly, your feet will face the same direction as your knee. You may have noticed throughout your life that you walked pigeon toed (feet facing towards each other) or walked more like a duck (feet facing outward). Now, it is wise to have a physical therapist check this status as you could simply have hip tightness which is giving a false positive that your hips are rotated. If that is the case you want to start walking and squatting with your feet and knees straight. If you have true hip anteversion or retroversion then a concession needs to be made about your feet placement. Get this checked out!
We need to check this out first!
Are you afraid that pushing your knees out wider than your feet is just as bad as allowing them to collapse together? Fear not! There are no anatomical structures that are in peril when we push the knees out wider than the feet during a squat.
Good Bad
The last aspect of squatting we will discuss is keeping the spine in neutral and trying to keep the spine as vertical as possible. Keeping the spine in neutral is a much safer position for the spine and forces the hips into more flexion. The hips are designed for this flexion and maximizing hip flexion keeps the glute muscles working properly. When the spine is more vertical during a squat the pressure on the lower lumbar discs decreases. This is a win-win!
Spine Neutral-YES! Spine Flexed-NO!
Outstanding!
I will conclude this part two on the Squat with some more images and then a final thought. The third and final installment of this series will elaborate on how to incorporate the squat into your exercise program.
No!
No!
Yes!
Yes!
Yes!
Yes!
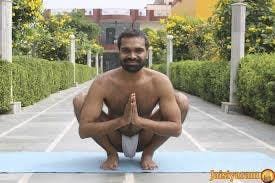
Why is it that non domesticated cultures squat so well? Maybe because they don’t know what a chair is. They probably don’t know what a TVA is, or a posterior glute medius nor an external oblique muscle. Why is that? Because they just simply squat as a sitting position. They don’t focus on reductionism nor muscle function. They simply squat be cause that’s what they have always done and if its not broke why fix it. They have not introduced chairs because, why bother, they already know how to sit. This begs the question- who is the more advanced society? The one who forces their society to sit in a non-functional way creating dysfunction? or the one who perpetuates challenging yet functional squatting in their culture? I’ll let you make up your own opinion.